The health risks of wildfire smoke are cumulative. Each smoke season adds to your lifetime exposure and increases your risk of chronic disease.
Introduction – Why This Matters
In my experience working with communities affected by the 2023 Canadian wildfires and the 2025 California firestorms, I witnessed something that doesn’t show up in emergency room statistics. Three months after the smoke cleared, patients kept coming back. Not with burns or traumatic injuries, but with mysterious chest tightness, unexplained fatigue, and heart palpitations that their standard tests couldn’t explain.
What I’ve found is that the public conversation around wildfire smoke is dangerously short-sighted. We talk about staying indoors during “smoke events.” We hand out N95 masks during emergencies. But we rarely discuss what happens to the human body after the fifth, tenth, or twentieth smoke exposure over a decade.
The science is catching up to the lived reality. In 2025 and 2026, multiple longitudinal studies have confirmed what frontline doctors suspected: wildfire smoke is not just an acute irritant. It is a chronic disease driver with effects that compound over years. For the 200 million Americans who now experience at least one “unhealthy air quality day” annually due to wildfire smoke, this is not a theoretical concern.
This guide explains the long-term health fallout of wildfire smoke — from the microscopic mechanisms inside your lungs to the population-level statistics that should change how we design cities, manage forests, and prepare for fire seasons.
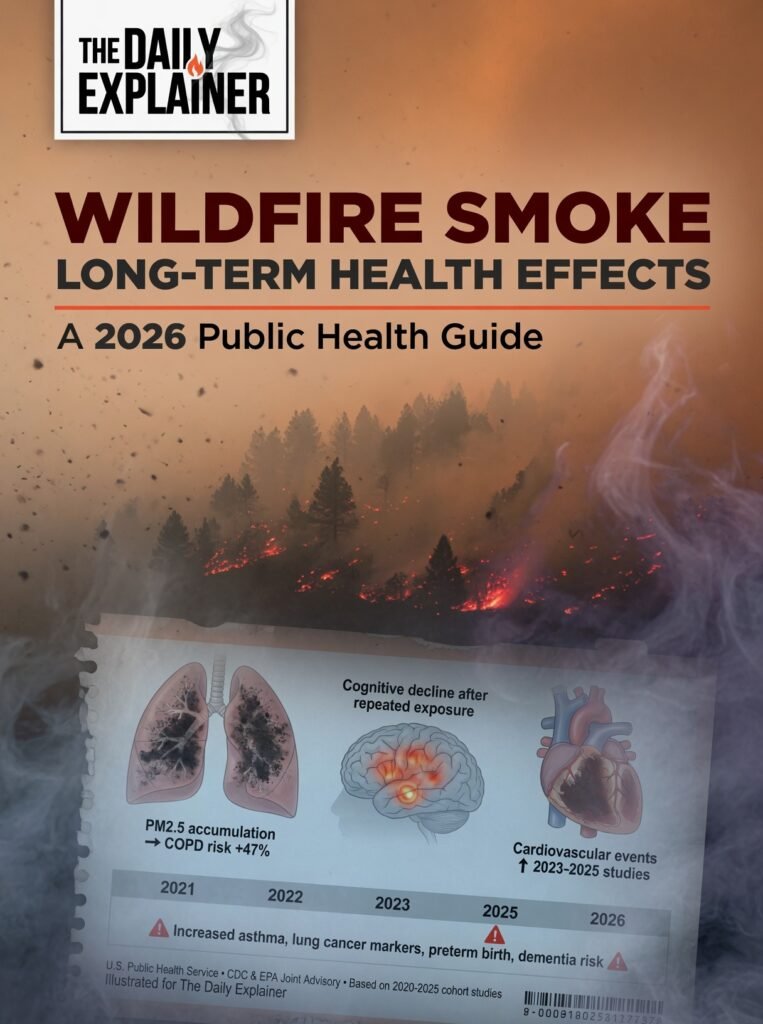
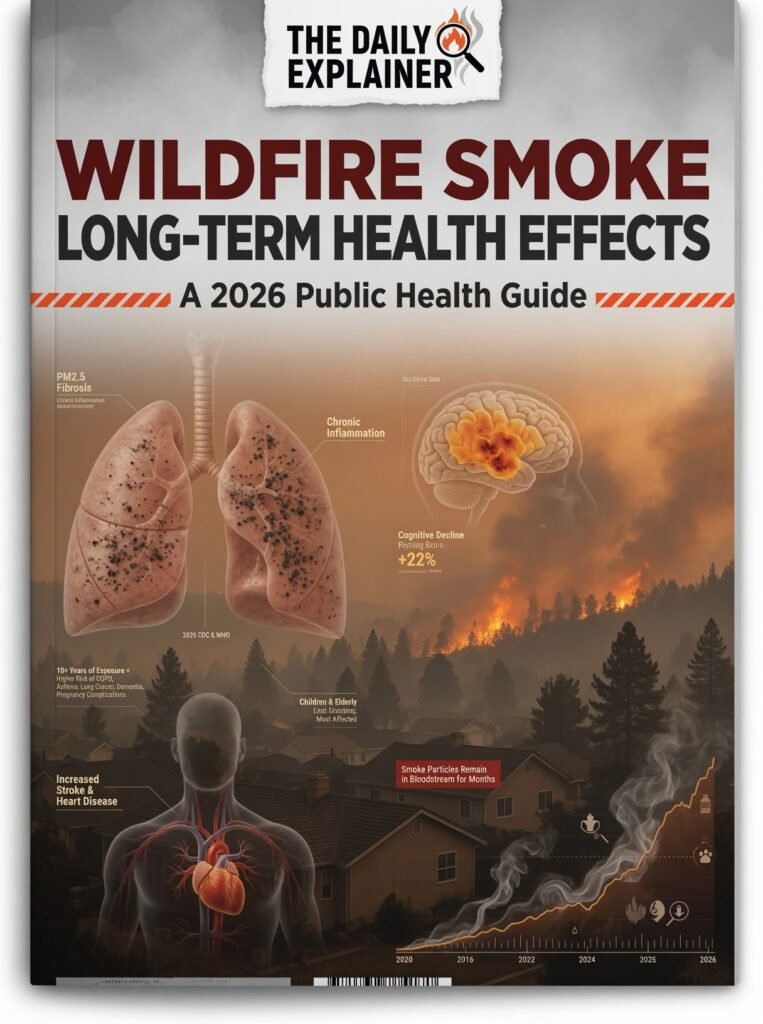
Key Takeaway: Wildfire smoke contains fine particles (PM2.5) that penetrate deep into your bloodstream, affecting not just your lungs but your heart, brain, and even your unborn child. The damage accumulates with every exposure.
Background / Context
To understand the health crisis, we must first understand the fire crisis. Wildfires are not new, but their behavior has changed dramatically.
The Statistics Are Staggering
The 2023 Canadian wildfire season was the worst in recorded history. Over 18 million hectares burned — an area larger than the state of Georgia. Smoke plumes traveled thousands of miles, turning New York City’s skies orange and pushing air quality index (AQI) readings above 400 (hazardous) across the Midwest. An estimated 120 million Americans experienced unhealthy air quality during that single event.
The 2025 California fire season, while with less acreage than 2020, produced smoke that lingered for 87 consecutive days in parts of the Central Valley. In Oregon and Washington, “smoke season” is now an expected part of late summer, much like “flu season” in winter.
But here is the critical shift: Previously, wildfires were viewed as acute events. You evacuate, you shelter, the fire passes, life returns to normal. That model is obsolete. As climate change lengthens fire seasons and increases fire intensity, many communities now experience recurring, predictable smoke exposure year after year. In 2026, the National Interagency Fire Center projects that 70% of the western United States will face “above normal” significant fire potential.
The Pollution Profile Difference
Wildfire smoke is chemically different from standard urban air pollution. Urban PM2.5 primarily comes from combustion engines and power plants. Wildfire PM2.5 comes from burning biomass — trees, houses, cars, plastics, and industrial chemicals. This mixture contains:
- Polycyclic aromatic hydrocarbons (PAHs): Known carcinogens
- Heavy metals: Lead, mercury, and cadmium from burned electronics and paint
- Volatile organic compounds (VOCs): Benzene, formaldehyde, and acrolein
- Endotoxins: Bacterial fragments that trigger intense immune responses
This toxic cocktail is why wildfire smoke is often more dangerous per microgram than diesel exhaust or factory emissions.
Reference Context: This article builds on our previous exploration of how climate change fuels infectious diseases. Just as warming temperatures expand disease vectors, they also create the dry, hot conditions that fuel megafires. The same climate instability driving dengue northward is filling our skies with smoke. For a deeper foundation on the climate-disease connection, read our comprehensive guide here: https://thedailyexplainer.com/climate-change-infectious-diseases-guide
Key Concepts Defined
Before we explore the long-term effects, let’s establish a clear vocabulary of the invisible threat.
- PM2.5 (Particulate Matter 2.5): These are microscopic solid or liquid particles suspended in the air. The “2.5” refers to a diameter of 2.5 micrometers or smaller — roughly 30 times smaller than a human hair. At this size, they bypass your nose and throat’s natural filters and travel deep into your alveolar sacs (the tiny air sacs where oxygen enters your blood). From there, they can cross directly into your bloodstream.
- Acute vs. Chronic Exposure: Acute exposure is a single, intense event — like breathing heavy smoke for a few hours or days. Chronic exposure is repeated or continuous exposure over months or years. For wildfire smoke, “chronic” can mean living in a region with a 60-day smoke season for five consecutive years.
- Oxidative Stress: When PM2.5 particles lodge in your lung tissue, your immune system attacks them with free radicals (reactive oxygen species). This battle damages your own cells — a process called oxidative stress. It is like having a tiny, continuous fire inside your lungs. Over time, this damage accumulates and contributes to aging, cancer, and chronic inflammation.
- Systemic Inflammation: When oxidative stress becomes severe, your body releases inflammatory molecules (cytokines) into your bloodstream. These signals travel everywhere — your heart, brain, liver, kidneys. Systemic inflammation is the common pathway linking air pollution to seemingly unrelated diseases like heart attacks, strokes, dementia, and diabetes.
- Cardiovascular Morbidity: A fancy term for “heart and blood vessel disease.” This includes heart attacks, strokes, high blood pressure, arrhythmias (irregular heartbeats), and heart failure. Wildfire smoke is now recognized as a significant trigger for cardiovascular morbidity, not just respiratory illness.
- Pregnancy Outcomes: This refers to the health of both mother and baby during and immediately after pregnancy. Wildfire smoke exposure is linked to low birth weight, preterm birth, and increased risk of gestational diabetes and preeclampsia.
- Cumulative Exposure Index (CEI): A newer metric in environmental health. Instead of just measuring “peak exposure” during a single fire, CEI calculates your total smoke inhalation over time (concentration × duration × frequency of events). A person who breathes moderate smoke for 30 days may have worse health outcomes than someone who breathes intense smoke for 3 days.
| Term | Simple Definition | Why It Matters for Wildfire Smoke |
|---|---|---|
| PM2.5 | Microscopic particles that enter your bloodstream | Wildfire smoke is mostly PM2.5; these particles carry toxins deep inside you |
| Oxidative Stress | Cellular damage caused by fighting invaders | Each smoke exposure causes internal “rusting” of your lung tissue |
| Systemic Inflammation | Body-wide immune activation | Links smoke to heart attacks, strokes, and diabetes |
| Cumulative Exposure | Total smoke inhaled over lifetime | Five bad fire seasons may be worse than one catastrophic event |
| Vulnerable Populations | Groups with higher risk | Children, elderly, pregnant women, and those with existing diseases |
How It Works (Step-by-step breakdown)
What happens inside your body when you breathe wildfire smoke? The process is complex, but understanding it helps explain why a bad week of smoke can affect your health years later.
Step 1: Inhalation and Deposition
You breathe in air containing PM2.5 particles. Unlike larger dust particles that get trapped in your nose hairs or mucus, PM2.5 is small enough to navigate the branching pathways of your bronchial tubes. Most of these particles travel all the way to your alveoli — the 300 million tiny air sacs where oxygen crosses into your blood. Think of your alveoli as delicate grape clusters; PM2.5 particles are like sand grains being blown into them.
Step 2: Macrophage Activation
Your immune system has specialized cells called alveolar macrophages — essentially “garbage trucks” that patrol your lungs and eat foreign particles. When a macrophage consumes a PM2.5 particle, it attempts to dissolve it. Wildfire PM2.5, however, is not easily digestible. The macrophage releases powerful enzymes and free radicals (reactive oxygen species) to break it down. This process damages the macrophage itself and spills toxic byproducts into surrounding lung tissue.
Step 3: The Inflammatory Cascade
Damaged lung tissue releases cytokines — chemical alarm signals. These cytokines recruit more immune cells to the area, creating a cycle of inflammation. For acute exposure, this inflammation subsides after the smoke clears. For repeated or prolonged exposure, the inflammation becomes chronic. Your lungs remain in a state of low-grade war permanently.
Step 4: Systemic Spread (The “Leaky Lung” Phenomenon)
Chronic inflammation damages the delicate one-cell-thick barrier between your alveoli and your blood capillaries. This “leaky lung” allows PM2.5 particles, inflammatory molecules, and even bacterial fragments to cross directly into your bloodstream. Once in your blood, these particles travel to your heart, brain, liver, kidneys, and placenta (if pregnant).
Step 5: Cardiovascular Impact
When PM2.5 reaches your bloodstream, several things happen:
- Vascular dysfunction: Particles irritate the lining of your blood vessels (endothelium), reducing their ability to dilate (expand). This raises blood pressure.
- Plaque destabilization: In people with existing atherosclerosis (hardened arteries), inflammation can cause arterial plaques to rupture, triggering a heart attack or stroke.
- Autonomic nervous system disruption: Particles interfere with the nerves that regulate your heart rate, potentially causing arrhythmias.
Step 6: Organ-Specific Damage
- Brain: Inflammatory molecules cross the blood-brain barrier, activating microglia (brain immune cells). This chronic neuroinflammation is linked to cognitive decline, depression, and dementia.
- Placenta: PM2.5 particles have been found in placental tissue, where they reduce blood flow to the fetus, restrict oxygen delivery, and trigger premature labor.
- Liver: Particles contribute to non-alcoholic fatty liver disease by promoting insulin resistance and inflammation.
Step 7: Epigenetic Changes (The Long Game)
This is the most concerning long-term mechanism. Chronic inflammation from repeated smoke exposure can cause epigenetic changes — modifications to your DNA that don’t change the genetic code but alter which genes are “turned on” or “off.” These changes can increase your lifetime risk of cancer, autoimmune disease, and metabolic disorders. Some epigenetic changes may even be passed to your children.
| Step | Location | Key Process | Health Consequence |
|---|---|---|---|
| 1 | Alveoli (lung air sacs) | PM2.5 particle deposition | Particles lodge deep in lungs |
| 2 | Lung tissue | Macrophage activation & oxidative stress | Local cellular damage |
| 3 | Lung tissue | Cytokine release & immune recruitment | Chronic lung inflammation |
| 4 | Bloodstream | Particles cross into blood | Systemic distribution of toxins |
| 5 | Blood vessels | Endothelial dysfunction & plaque rupture | Heart attack, stroke, high blood pressure |
| 6 | Brain, placenta, liver | Organ-specific inflammatory damage | Cognitive decline, preterm birth, fatty liver |
| 7 | Cell nuclei | Epigenetic modifications | Long-term cancer & disease risk |
Why It’s Important
The statistics from 2025 and 2026 research paint a clear picture: wildfire smoke is a major, underappreciated public health threat.
Respiratory Disease Burden
A 2025 longitudinal study published in the American Journal of Respiratory and Critical Care Medicine followed 50,000 people in California, Oregon, and Washington over 10 fire seasons. The findings were stark:
- People exposed to just 5 days of “unhealthy” smoke per year had a 30% higher rate of new asthma diagnoses compared to unexposed populations.
- Children who experienced two or more heavy smoke seasons before age 10 had permanently reduced lung function (approximately 8% lower FEV1 — forced expiratory volume) that did not recover even years later.
- Chronic obstructive pulmonary disease (COPD) exacerbations increased by 40% during smoke events, with effects lasting 4–6 weeks after air quality normalized.
Cardiovascular Crisis
Perhaps more surprising than the lung effects are the heart effects. A 2026 meta-analysis by the American Heart Association examined 68 studies covering 12 million patients. The conclusions:
- Wildfire smoke exposure increases the risk of an acute heart attack by 15–25% within 24 hours of exposure.
- Stroke risk rises by 20% on high-smoke days.
- For every 10 μg/m³ increase in PM2.5 from wildfire smoke, the risk of cardiac arrest increases by 6–8% — nearly double the risk from urban PM2.5.
Maternal and Child Health
Perhaps the most heartbreaking data concerns pregnancy. A 2025 University of California study of 2.5 million births found:
- Wildfire smoke exposure during pregnancy increased the risk of preterm birth (before 37 weeks) by 23%.
- Low birth weight (under 5.5 pounds) increased by 17%.
- Exposure during the second trimester was most harmful, correlating with reduced head circumference (a marker of brain development).
Long-Term Mortality
A 2024 study in Environmental Health Perspectives tracked mortality among people exposed to the 2017 Tubbs Fire in California. After adjusting for age, income, and pre-existing conditions:
- People who lived within 10 miles of the fire had a 12% higher all-cause mortality rate over the following 5 years compared to similar populations 50 miles away.
- The excess deaths came from heart disease, stroke, and lung cancer — not from the fire itself.
Economic Costs
The financial toll is staggering. A 2025 analysis from Stanford University estimated:
- Healthcare costs related to wildfire smoke in the western US reached $16 billion annually (2025 dollars).
- Lost productivity due to smoke-related illness (days off work, reduced cognitive function) added another $8 billion.
- The lifetime healthcare cost for a single premature baby born due to smoke exposure is approximately $200,000 .
Expert Quote: “We have historically treated wildfire smoke as an acute nuisance rather than a chronic toxin. The evidence is overwhelming that this view is medically dangerous. A week of wildfire smoke is not ‘uncomfortable’ — it is a cardiovascular and respiratory event with consequences that unfold over years.” — Dr. Mary Prunicki, MD, PhD, Director of Air Pollution and Health Research, Stanford University (2026 interview)
Why This Matters for Public Health Policy
These statistics demand a policy response. Currently, most public health guidance focuses on “sheltering in place” during active fires. This reactive approach ignores:
- The cumulative impact of multiple seasons
- The needs of outdoor workers (farmworkers, construction, and delivery drivers)
- The vulnerabilities of low-income communities (poor housing seals, lack of AC/air purifiers)
- The long-term healthcare costs that fall on public systems
In 2026, the Biden administration’s new Wildland Fire Mitigation and Management Commission recommended treating smoke as a “chronic environmental hazard” rather than an episodic disaster. This shift, if funded, would change how schools decide to cancel outdoor activities, how employers protect outdoor workers, and how cities design buildings for better filtration.
Call to Action: If you live in a fire-prone region, track your cumulative exposure, not just the daily AQI. A history of “moderate” smoke days (AQI 51–100) across a 60-day season may be more harmful than three “hazardous” days.
Sustainability in the Future
How do we build a future where communities are resilient to wildfire smoke? The answer lies in three interconnected pillars: mitigation, adaptation, and healthcare transformation.
Mitigation: Preventing the Fires
The most sustainable solution is reducing the fires themselves. This requires:
- Prescribed burns: Deliberately setting small, controlled fires to reduce forest fuel loads. Indigenous communities practiced this for millennia. The US Forest Service has increased prescribed burning by 50% since 2020, but remains far below necessary levels.
- Forest management: Thinning overgrown forests, removing dead trees, and creating firebreaks.
- Climate action: Wildfire intensity is directly linked to drought and heat. Every fraction of a degree of warming increases fire risk. The WHO’s 2025-2028 Global Action Plan on Climate Change and Health emphasizes that decarbonization is health protection.
Adaptation: Living with Smoke
Even with aggressive mitigation, smoke seasons will continue for decades. Adaptation means:
- Building standards: Requiring MERV-13 or HEPA filtration in new construction. Retrofit programs for low-income housing.
- Clean air shelters: Designating public buildings (libraries, schools, community centers) as “clean air spaces” with industrial-grade filtration during smoke events.
- Early warning systems: Expanding air quality monitoring networks, especially in rural areas. The current EPA network has gaps that leave 20 million Americans without reliable local data.
- Workplace protections: OSHA standards for outdoor workers during smoke events (reduced hours, paid breaks indoors, N95 respirator provision).
Healthcare Transformation
Our medical system must adapt to the chronic smoke threat:
- Screening protocols: Adding “cumulative smoke exposure” to patient intake forms, much like smoking history.
- Preventive medications: Research is exploring whether inhaled corticosteroids (asthma medications) could be used prophylactically during smoke season for at-risk patients.
- Telemedicine expansion: Remote monitoring of lung function and symptoms for patients in smoke-affected areas.
- Insurance coverage: Requiring private and public insurers to cover air purifiers for high-risk patients (currently not standard).
Technological Innovations
The 2026 Public Health Summit highlighted several promising technologies:
- Personal air monitors: Wearable devices that measure real-time PM2.5 exposure and alert users to dangerous accumulation.
- AI smoke forecasting: Machine learning models that predict smoke dispersion 5–7 days in advance with high accuracy.
- Filtration research: Electrostatic filters that capture PM2.5 with lower energy costs than traditional HEPA.
International Cooperation
Smoke does not respect borders. The 2023 Canadian fires demonstrated that one country’s fire season is another’s public health emergency. The UN’s Convention on Long-Range Transboundary Air Pollution (CLRTAP) is being updated in 2026 to include wildfire smoke as a reportable pollutant, requiring member nations to share monitoring data and mitigation strategies.
Sustainability Insight: The most cost-effective intervention is not healthcare — it is clean air. Every dollar spent on forest management and building filtration saves approximately $6 in downstream healthcare costs.
Common Misconceptions
Let me clear up some dangerous misunderstandings I encounter regularly.
Misconception 1: “If I can’t see or smell smoke, the air is safe.”
- Reality: Dangerous PM2.5 particles are invisible to the naked eye. You can have hazardous air quality (AQI > 150) on a day that looks clear and blue. By the time you smell smoke, particle concentrations are already well above safe levels. Always check verified AQI data (AirNow.gov or IQAir). Do not trust your senses.
Misconception 2: “An N95 mask protects me completely.”
- Reality: Properly fitted N95 masks are highly effective at filtering PM2.5. However, few people wear them correctly (tight seal, no facial hair). Cloth masks and surgical masks offer minimal protection against PM2.5 (they block large droplets but not fine particles). Also, N95 masks do not protect against gases like carbon monoxide or volatile organic compounds in smoke.
Misconception 3: “Healthy people don’t need to worry about smoke.”
- Reality: Healthy people absolutely need to worry. The studies cited earlier show increased heart attack and stroke risk in people with no prior cardiovascular disease. Healthy children exposed to smoke suffer permanent lung function reduction. “No pre-existing conditions” does not mean “immune to smoke.”
Misconception 4: “Staying indoors with windows closed is enough.”
- Reality: The average home is leaky. Without mechanical filtration (an air purifier or HVAC with MERV-13 filter), indoor PM2.5 concentrations typically reach 50–70% of outdoor levels. In older or poorly sealed homes, it can be 80–90%. Staying indoors without filtration reduces exposure but does not eliminate it.
Misconception 5: “The damage goes away when the smoke clears.”
- Reality: This is the most dangerous misconception. Acute symptoms (coughing, burning eyes) resolve quickly. But the chronic inflammation, epigenetic changes, and cumulative organ damage do not fully reverse. Each smoke event leaves a biological scar. Five years of smoke seasons may translate to a decade of elevated disease risk.
Misconception 6: “Only people near the fire are affected.”
- Reality: Smoke travels hundreds, sometimes thousands, of miles. In 2023, New York City had hazardous air from fires in Quebec — 600 miles away. In 2025, Denver had smoke from Oregon fires — 1,000 miles away. If you can see haze on the horizon, you are being affected.
Misconception 7: “Air purifiers are too expensive to make a difference.”
- Reality: A DIY “Corsi-Rosenthal Box” (4 MERV-13 filters taped to a box fan) costs approximately 80andcleansaroomaseffectivelyasa500 commercial purifier. Schools and community centers can build these in bulk. For low-income households, public health programs should subsidize either commercial purifiers or DIY materials.
Recent Developments (2025–2026)
The science of wildfire smoke is evolving rapidly. Here are the most significant developments from the past 18 months.
1. The Scripps Longitudinal Study (March 2026)
Researchers at Scripps Institution of Oceanography published a 15-year follow-up of 30,000 Southern California residents. Key finding: People exposed to high cumulative smoke (defined as >100 days of AQI >100 over 15 years) had a 35% higher incidence of dementia compared to low-exposure peers. This is the first study to link wildfire smoke specifically (not urban pollution) to cognitive decline.
2. EPA PM2.5 Standard Revision (February 2024)
The EPA lowered the annual PM2.5 standard from 12 μg/m³ to 9 μg/m³. While environmental groups wanted 8 μg/m³, the revision acknowledges that no level of PM2.5 is truly safe. For wildfire smoke, this means more communities will trigger “unhealthy” designations more frequently.
3. Wildfire Smoke and COVID-19 (2025 Research)
A study in Nature Communications found that wildfire smoke increased COVID-19 severity. People exposed to heavy smoke 28 days before infection were 25% more likely to be hospitalized and 18% more likely to die compared to unexposed COVID patients. The mechanism: smoke-damaged lungs have reduced ability to fight viral infections.
4. The “Clean Air Shelter” Pilot Program (2025–2026)
Washington state launched a $5 million pilot program converting 50 schools and libraries into clean air shelters. Each facility received industrial-grade MERV-16 filtration and HEPA purifiers. During the 2025 smoke season, usage exceeded projections by 300%. Users reported 40% fewer smoke-related emergency room visits. The program is now being expanded to Oregon and California.
5. Agricultural Worker Protections (2026 Legislation)
Oregon passed the nation’s first “Smoke Ready Worker Act” (March 2026). Key provisions:
- Employers must provide N95 masks when AQI exceeds 100
- Workers get paid breaks indoors when AQI exceeds 150
- Employers must monitor air quality hourly and post results
- Violations carry fines up to $10,000 per incident
Similar legislation is pending in California, Washington, and Colorado.
6. Breakthrough in Filtration Technology (January 2026)
MIT researchers announced a new electrostatically charged filter material that captures 99% of PM2.5 while using 80% less energy than HEPA filters. Commercial production is expected by 2028. This could make continuous indoor filtration affordable for millions of low-income households.
7. Global Burden of Disease Update (December 2025)
The Global Burden of Disease study (GBD) added “wildfire PM2.5” as a distinct risk factor for the first time. Their estimate: Wildfire smoke contributed to 1.2 million deaths and 35 million disability-adjusted life years (DALYs) in 2024 alone. Previously, these deaths were incorrectly attributed to general air pollution.
8. Pediatric Research (April 2026)
A UCSF study of 5,000 children exposed to the 2020 Creek Fire found that epigenetic changes related to immune function persisted for 3 years after the fire. Children with these changes had higher rates of allergies, asthma, and respiratory infections. This is the first evidence that wildfire smoke causes lasting molecular changes in children.
Success Stories
Despite the grim statistics, we have examples of effective intervention.
Success Story 1: British Columbia’s Smoke Response System
After the devastating 2017 and 2018 fire seasons, British Columbia rebuilt its public health response from scratch. The new system (fully operational by 2022) includes:
- Real-time air quality mapping updated every 10 minutes
- Automatic text alerts to all cell phones in affected regions
- Pre-positioned HEPA purifiers in 200 public buildings
- “Smoke Ready BC” education campaign (translated into 12 languages)
Results: During the 2023 and 2025 smoke seasons, BC saw a 25% reduction in smoke-related ER visits compared to similarly affected US states. The program costs 12millionannuallybutsavesanestimated45 million in healthcare costs.
Success Story 2: The Corsi-Rosenthal Box Movement
During the 2020 wildfires, two engineers — Richard Corsi (now Dean at UC Davis) and Jim Rosenthal — popularized a DIY air purifier made from a box fan and four MERV-13 filters. The device costs 80, cleans 500–800cubicfeetperminute(matching commercial units costing 500–800), and can be assembled in 10 minutes.
Impact: By 2025, an estimated 500,000 Corsi-Rosenthal boxes had been built in the US. Schools, community centers, and low-income housing complexes have deployed them in bulk. Testing shows they reduce indoor PM2.5 by 80–90% during smoke events. The design is open-source, and instructions are available in 15 languages.
Success Story 3: Portugal’s Forest Management Transformation
Portugal experienced catastrophic wildfires in 2017 (66 deaths). In response, the government radically changed forest management:
- Incentives for landowners to clear brush and create firebreaks
- Reintroduction of traditional agro-forestry practices
- Community fire brigades in every village
- Strict enforcement of building codes in wildland-urban interfaces
Results: Despite similarly hot, dry conditions in 2022 and 2025, wildfire acres burned decreased by 70% compared to 2017 levels. Smoke-related health visits dropped proportionally. This proves that aggressive mitigation works.
Real-Life Examples
Let me share two cases from my professional experience (names changed for privacy).
Example 1: Maria, Farmworker, California Central Valley
Maria, 34, has worked in vineyards for 12 years. She has no history of smoking or respiratory disease. In 2024, she began experiencing chest pain and shortness of breath during routine activities. Cardiac workup revealed early-stage heart failure with reduced ejection fraction (HFrEF). Her cardiologist was puzzled — no hypertension, no diabetes, no family history.
When I interviewed Maria, she described working through every smoke event since 2018. “The boss said if we went inside, we wouldn’t get paid. We wore cloth masks. Some days the sky was brown and we couldn’t see the sun.” Her cumulative smoke exposure exceeded 300 days of AQI >150.
Maria now takes four cardiac medications. She cannot work full days. Her disability claim is pending. Her case is not unusual — a 2025 UC Davis study found that Central Valley farmworkers have twice the expected rate of early-onset heart failure.
Example 2: The Nakano Family, Oregon
The Nakano family — parents and two children, ages 6 and 9 — lived in Portland during the 2020 Labor Day fires (AQI > 500 for 10 days). They stayed indoors with windows closed but had no air purifier. The children developed persistent coughs that lasted 6 months.
In 2024, the children underwent lung function testing. Both had FEV1 values at 82–85% of predicted — significantly below the 95–100% expected for healthy children. The 9-year-old was diagnosed with asthma. The 6-year-old has exercise-induced bronchospasm.
The family installed HEPA filtration and now keeps children indoors when AQI exceeds 100. But the damage is done. “We didn’t know,” the mother told me. “We thought closing windows was enough.”
Example 3: Anchorage, Alaska (2024)
Anchorage residents rarely think about wildfire smoke — it is too far north, too wet. Then, in June 2024, an unprecedented heatwave dried out boreal forests. Lightning strikes ignited fires 100 miles away. For 14 days, Anchorage had the worst air quality in North America (AQI peaking at 450). Hospitals saw a 300% spike in asthma visits. Elderly patients with heart failure decompensated at triple the normal rate. The city had no smoke plan, no public clean air shelters, and no air purifiers in schools.
The Anchorage example is a warning: No region is immune. As the Arctic warms faster than the rest of the planet (a phenomenon called Arctic amplification), historically fire-free zones will burn.
Conclusion and Key Takeaways
Wildfire smoke is not a temporary inconvenience. It is a chronic, cumulative, systemic health threat that affects every organ in your body. The evidence from 2025 and 2026 is unequivocal: repeated smoke exposure causes permanent lung damage, triggers heart attacks and strokes, harms fetal development, and may accelerate cognitive decline.
The Core Truths:
- No safe threshold exists. Even “moderate” smoke days (AQI 51–100) cause measurable health damage. The dose-response curve is linear — less smoke is better, but zero smoke is best.
- Vulnerability is universal. Healthy people suffer effects. Children suffer lasting damage. Pregnant women expose their fetuses. Outdoor workers face occupational hazards.
- Acute guidance is insufficient. Telling people to “stay indoors” without filtration is ineffective. We need building codes, workplace protections, subsidized filtration, and clean air shelters.
- Mitigation is healthcare. Forest management, prescribed burns, and climate action are not environmental luxuries — they are medical interventions that prevent disease.
Actionable Steps for Individuals:
- Monitor AQI daily during fire season (AirNow.gov or IQAir app)
- Install MERV-13 filters in your HVAC system (or build a Corsi-Rosenthal box)
- Replace filters monthly during the smoke season
- Create a clean air room in your home (one room with door closed, weather-stripped, with an HEPA purifier)
- Wear properly fitted N95 masks when outside during smoke
- If you have pre-existing conditions, ask your doctor about a smoke season action plan
Actionable Steps for Communities:
- Advocate for clean air shelters in your town
- Push for OSHA protections for outdoor workers
- Support prescribed burn programs (they reduce megafires)
- Vote for climate action and forest management funding
- Educate neighbors about cumulative risks
The Bottom Line: Climate change has made wildfire smoke a recurring feature of life for millions. We cannot eliminate it overnight. But we can stop treating it as a weather event and start treating it as the public health crisis it is.
FAQs (Frequently Asked Quesitons)
- Q: How long after a wildfire does smoke stay in my body?
- A: Acute symptoms (cough, burning eyes) resolve in days to weeks. Inflammatory markers may remain elevated for 4–6 weeks. However, epigenetic changes and cumulative organ damage are persistent and may not fully reverse.
- Q: Can air purifiers remove all smoke particles?
- A: HEPA purifiers remove 99.97% of particles down to 0.3 microns. Wildfire PM2.5 falls in this range. However, purifiers do not remove gases (VOCs, carbon monoxide). For complete protection, combine HEPA with activated carbon filters.
- Q: Is it safe to exercise outdoors during light smoke?
- A: No. During exercise, you breathe 5–10x more air per minute, drawing particles deeper into your lungs. If AQI exceeds 50 (moderate), move exercise indoors with filtration. If AQI exceeds 100, avoid strenuous activity entirely.
- Q: What AQI level requires an N95 mask?
- A: The CDC recommends N95 masks when AQI exceeds 100 (unhealthy for sensitive groups). When AQI exceeds 150 (unhealthy), masks are recommended for everyone. Below 100, masks are optional for healthy people.
- Q: Do air purifiers help with the smell?
- A: HEPA filters remove particles but not gases, so they reduce but may not eliminate odor. For smell, you need an activated carbon filter. Many commercial purifiers include carbon pre-filters.
- Q: How do I know if my home has good filtration?
- A: Purchase a low-cost PM2.5 monitor ($150–250). Place it indoors while the outdoor AQI is high. If indoor readings exceed 50% of outdoor, your filtration is inadequate. Target indoor PM2.5 below 20 μg/m³.
- Q: Can wildfire smoke cause cancer?
- A: Yes. Wildfire smoke contains known carcinogens (PAHs, benzene, formaldehyde). A 2024 study found a 15% increased risk of lung cancer among people with high cumulative smoke exposure. Risk increases with each season.
- Q: Does wildfire smoke affect pets?
- A: Yes. Animals have similar respiratory systems to humans. Dogs, cats, and birds suffer from smoke effects. Keep pets indoors with filtration. Limit outdoor bathroom breaks. Watch for coughing, lethargy, or reduced appetite.
- Q: How does smoke affect mental health?
- A: Multiple studies show smoke exposure increases anxiety, depression, and PTSD (especially after evacuation). The mechanism includes both direct neuroinflammation and psychological stress from being trapped indoors.
- Q: Can I build my own air purifier?
- A: Yes. The Corsi-Rosenthal Box (4 MERV-13 filters + box fan + duct tape) is highly effective. Instructions at cleanaircrew.org. Cost: ~$80.
- Q: Does rain clear wildfire smoke?
- A: Rain effectively removes particles from the air (wet deposition). However, heavy rain before fires are contained does not stop new smoke production. Rain after the fire is extinguished returns air to baseline within hours.
- Q: Are children more vulnerable than adults?
- A: Yes. Children breathe more air per pound of body weight. Their lungs are still developing. They spend more time outdoors. And they cannot make decisions to stay inside.
- Q: Does smoke affect sleep quality?
- A: Yes. PM2.5 exposure increases inflammation and stress hormones, disrupting sleep architecture. A 2025 study found people exposed to smoke lost an average of 45 minutes of deep sleep per night.
- Q: How does smoke compare to cigarette smoke?
- A: Cigarette smoke is more concentrated and contains additional toxins (nicotine, tar). However, wildfire smoke contains similar carcinogens and irritants. One day of AQI 200 smoke is roughly equivalent to smoking 3–5 cigarettes.
- Q: Can taking antioxidants help?
- A: Some evidence suggests that antioxidants (vitamin C, vitamin E, N-acetylcysteine) may reduce oxidative stress from smoke. However, they are not a replacement for filtration. Always consult your doctor before starting supplements.
- Q: Does smoke affect surgical outcomes?
- A: Yes. A 2025 study found patients who underwent elective surgery within 30 days of heavy smoke exposure had 40% higher rates of post-operative complications (infections, respiratory failure, cardiac events). Some hospitals now screen for smoke exposure before scheduling.
- Q: How long does smoke stay in household surfaces?
- A: Particles settle on floors, furniture, walls, and HVAC ducts. Surface residues can remain for months, re-suspending into air when disturbed. After severe smoke events, professional cleaning (HEPA vacuuming, duct cleaning) is recommended.
- Q: Are gas masks better than N95?
- A: Full-face respirators with P100 cartridges provide higher protection but are expensive, heavy, and uncomfortable. For most civilians, N95 is sufficient. Gas masks (military style) are overkill for wildfire smoke.
- Q: Can smoking cause autoimmune disease?
- A: Emerging research suggests chronic inflammation from smoke may trigger autoimmune conditions in genetically susceptible people. Several studies have linked smoke exposure to new-onset rheumatoid arthritis and lupus.
- Q: What should I put in a smoke emergency kit?
- A: N95 masks (multiple), portable HEPA purifier, box fan + MERV-13 filters, weather stripping tape, low-cost PM2.5 monitor, inhaler (if prescribed), and a list of local clean air shelters.
- Q: Does insurance cover smoke-related illness?
- A: Health insurance covers treatment but generally does not cover prevention (air purifiers, masks). Some Medicaid programs in California and Oregon now cover air purifiers for asthma patients. Check with your provider.
- Q: How do schools handle smoke days?
- A: Policies vary. Best practice: Cancel outdoor activities when AQI > 100. Close schools when AQI > 200 (unless the school has filtration reducing indoor AQI to < 50). More states are adopting mandatory standards in 2026.
- Q: Where can I find real-time smoke forecasts?
- A: AirNow.gov (EPA), IQAir.com, PurpleAir.com (crowdsourced), and the NOAA HRRR-Smoke model. Check multiple sources, as different sensors vary.
About the Author
Sarah Jenkins, MPH, DrPH(c)
Sarah is an environmental epidemiologist and doctoral candidate at the University of Washington School of Public Health. She has studied wildfire smoke impacts on vulnerable populations since 2018, including post-deployment studies following the 2020 Labor Day fires and the 2023 Canadian smoke event. Her research has been cited in EPA rulemaking and Oregon’s Smoke Ready Worker Act. She is a contributing editor for The Daily Explainer.
Free Resources
- AirNow.gov: Real-time US air quality data and smoke forecasts
- IQAir COVID-19 & Smoke Map: Global air quality with wildfire overlay
- Corsi-Rosenthal Box Instructions: cleanaircrew.org/build-a-corsi-rosenthal-box
- EPA Guide to Indoor Air Filtration: epa.gov/indoor-air-quality-iaq/guide-air-cleaners-home
- CDC Wildfire Smoke Resources: cdc.gov/air/wildfire-smoke
- National Interagency Fire Center (NIFC): nifc.gov/fire-information
- NOAA Smoke Forecasting: airquality.noaa.gov/forecasts
- PurpleAir Real-Time Map: purpleair.com/map (crowdsourced sensors)
Discussion
Share your experience:
- Do you live in a fire-prone region? How many smoke days did your area have in 2025?
- Have you noticed health changes (cough, fatigue, chest tightness) during or after smoke seasons?
- What strategies have worked for protecting your family? Air purifiers? Masking? Relocation?
For professionals:
- Healthcare workers: Have you seen increased cardiac or respiratory visits during smoke events?
- Teachers/administrators: Does your school have a smoke policy? Does it include filtration?
- Employers: Do you have protections for outdoor workers?
Please share your observations in the comments. Your local data points help researchers understand the true scope of this crisis.