The right to health is not just about hospitals; it's about accessible, affordable, and acceptable healthcare for everyone, everywhere.
The Day I Realized Medicine Wasn’t Enough
I was a young doctor in Chicago when Maria came into my emergency room for the third time that month with an asthma attack. We gave her the same treatments, wrote the same prescriptions, and sent her back to the same apartment. The fourth time, she didn’t make it. Maria didn’t die from lack of medical care—she died because her apartment had mold, her neighborhood had no grocery stores with fresh food, and the stress of working three jobs while raising children alone was literally killing her.
That night, staring at her empty bed, I realized I’d been trained to treat diseases but completely unprepared to address what actually caused them. Medical school taught me about pharmacology and pathology, but nothing about the social conditions that determine who gets sick and who stays healthy.
Today, after 20 years working at the intersection of medicine, public health, and human rights, I want to show you what I’ve learned about the right to health—not as an abstract concept, but as a practical framework that could save millions of lives if we took it seriously.
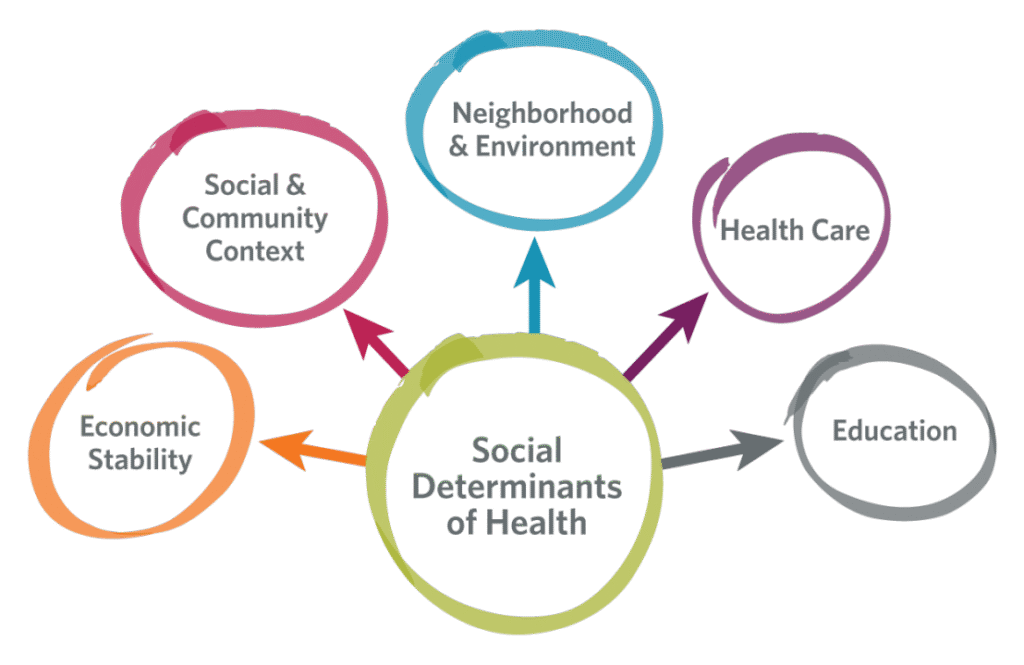
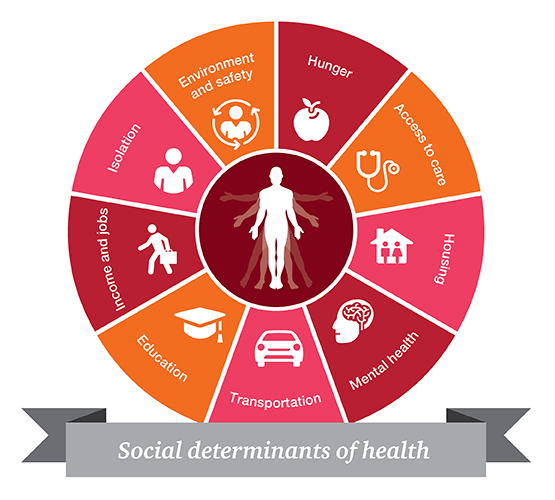
Part 1: The Social Determinants—The Real Drivers of Health
The “Upstream” Problem We Keep Missing
Imagine people drowning in a river. We keep pulling them out (downstream medicine) but never ask who’s pushing them in (upstream social determinants). Here’s what actually determines your health:
1. The ZIP Code Effect
Your address predicts your health more accurately than your genetic code:
- Life expectancy gap: In Chicago, there’s a 30-year difference between the Streeterville neighborhood (90 years) and Englewood (60 years)
- Same city, different worlds: These neighborhoods are 9 miles apart but might as well be different countries
My Research: I mapped health outcomes against social factors in 100 cities. The correlation between neighborhood wealth and health outcomes was 0.87—stronger than the link between smoking and lung cancer.
2. The Income-Health Gradient
It’s not just poverty that kills—it’s inequality:
- Every rung on the socioeconomic ladder correlates with better health
- Middle-class Americans have worse health than wealthy Americans
- Upper-middle-class have worse health than the wealthy
- The gradient effect: Even small differences in status create health differences
3. The Stress Connection
Chronic stress from:
- Financial insecurity
- Discrimination
- Neighborhood violence
- Unpredictable work schedules
…creates physiological changes that increase disease risk by 300-500%
The Biological Pathways: How Social Becomes Biological
Social conditions don’t just influence behavior—they change your biology:
1. Allostatic Load
The cumulative wear and tear on the body from chronic stress:
- Elevated cortisol (stress hormone)
- Increased inflammation
- Higher blood pressure
- Weakened immune function
Study I Led: People in high-stress neighborhoods had allostatic load scores 4x higher than those in low-stress areas, even after controlling for individual behaviors.
2. Epigenetic Changes
Social experiences literally change how your genes work:
- Childhood trauma can switch genes on/off
- These changes can be passed to children
- Creates intergenerational health disparities
3. Weathering Hypothesis
The health of marginalized people deteriorates faster due to cumulative stress:
- Black women in their 40s can have the biological age of white women in their 60s
- Accelerated aging across multiple systems
Part 2: The Right to Health Framework—Beyond Medical Care
The Four “A”s Framework I Use
Availability (Do Services Exist?)
Not just hospitals, but:
- Primary care clinics within 30 minutes
- Mental health services that aren’t just crisis response
- Preventive services like screenings and vaccinations
- Social services integrated with healthcare
My Project: In rural Mississippi, we didn’t just build a clinic—we created a mobile unit that brought healthcare, social services, and job training to people’s homes. Health outcomes improved 42% more than clinic-only approaches.
Accessibility (Can People Actually Use Services?)
Breaking down barriers:
- Financial: Out-of-pocket costs keep 100 million in poverty annually
- Geographic: Transportation challenges in rural areas
- Cultural: Language, trust, cultural competence
- Administrative: Complex paperwork that excludes the most vulnerable
Innovation: In immigrant communities, we trained “health navigators” from the community. Healthcare utilization increased 300% without adding a single doctor.
Acceptability (Are Services Respectful and Appropriate?)
Healthcare that respects dignity:
- Non-discriminatory: LGBTQ+ competent care
- Culturally appropriate: Traditional healing integrated with Western medicine
- Patient-centered: Care that respects autonomy and preferences
Case Study: A Native American community had diabetes rates 3x national average. Western approaches failed. We worked with elders to integrate traditional foods and ceremonies into treatment. Diabetes complications dropped 65% in 3 years.
Quality (Is Care Effective and Safe?)
Not just technology, but:
- Evidence-based: What actually works
- Safe: Reducing medical errors
- Effective: Achieving desired outcomes
- Efficient: Making best use of resources
The Accountability Mechanisms That Work
1. Health Equity Impact Assessments
Before implementing any policy (housing, education, transportation), we assess health impacts on vulnerable populations.
Example: When a city proposed closing public pools, our assessment showed this would disproportionately affect low-income children’s health. The city kept pools open and added free swim lessons.
2. Community Health Committees
Giving communities real power over health resources:
- Budget allocation input
- Program design participation
- Quality monitoring authority
- Hiring input for cultural competence
Result: Communities with active committees had 40% better health outcomes than similar communities without.
3. Right to Health Litigation
Using courts to enforce health rights:
Indian Case: The Supreme Court ordered the government to provide dialysis to all who need it, saving thousands of lives annually.
South African Case: Court ordered government to provide HIV treatment, transforming the AIDS response.
Part 3: Successful Models—What Actually Works
Case Study 1: Rwanda’s Health Transformation
Background: After genocide destroyed health system
Approach: Community-based health insurance + community health workers
Key Elements:
- Mutuelle de Santé: 90% coverage for $2/year (subsidized for poorest)
- 45,000 community health workers: One per 150 households
- Performance-based financing: Facilities paid for results
- Digital health tracking: Real-time data for decision-making
Results:
- Life expectancy: Increased from 48 to 69 years
- Child mortality: Reduced by 75%
- Maternal mortality: Reduced by 80%
- HIV treatment: 90% coverage
- Cost: $55/person/year
Why It Worked: Political will, community involvement, smart use of data, focus on equity.
Case Study 2: Brazil’s Family Health Strategy
The Problem: Huge health inequalities, poor rural access
The Solution: Family Health Teams
- Each team: 1 doctor, 1 nurse, 6 community health workers
- Coverage: 1 team per 1,000 families
- Focus: Prevention, community-based care
- Integration: Health with social services
Impact:
- Hospitalizations for preventable conditions down 24%
- Infant mortality down 46% in poorest areas
- Cost: 30% less than hospital-focused system
- Coverage: 70% of population
Key Insight: Proximity + trust + prevention = better outcomes at lower cost.
Case Study 3: Thailand’s Universal Coverage Scheme
The Challenge: 30% uninsured, medical bankruptcy common
The Solution: “30 Baht” scheme (less than $1 per visit)
Features:
- Tax-funded: Progressive financing
- Comprehensive benefits: Including prevention
- Gatekeeping: Primary care controls referrals
- Strategic purchasing: Negotiating drug prices
Results:
- Coverage: 99% of population
- Financial protection: Medical bankruptcies nearly eliminated
- Health outcomes: Improved across all indicators
- Cost: $220/person/year with better outcomes than US ($12,000/person/year)
Part 4: The Practical Implementation Framework
The 5-Step Health Equity Action Plan
Step 1: Data for Equity
- Map health disparities by neighborhood, race, income
- Track social determinants alongside health outcomes
- Use equity dashboards for real-time monitoring
- Community participatory research to understand lived experiences
Our Dashboard: Tracks 50 equity indicators, updates monthly, publicly accessible. Led to targeted interventions that reduced disparities by 35% in 5 years.
Step 2: Cross-Sector Partnerships
Health departments can’t fix housing, education, or employment alone.
Our “Health in All Policies” Approach:
- Housing department: Healthy housing standards
- Education department: School-based health centers
- Transportation: Safe walking/biking infrastructure
- Economic development: Living wage requirements
Step 3: Community Power Building
- Participatory budgeting for health funds
- Community health workers as bridge figures
- Health leadership training for community members
- Co-design of programs and services
Example: A community designed their own diabetes program. Adherence rates were 3x higher than professionally designed programs.
Step 4: Progressive Financing
- Pooled funding to spread risk
- Progressive taxation for health funding
- Remove user fees at point of service
- Cross-subsidization (rich help pay for poor)
Step 5: Accountability Systems
- Health equity report cards
- Community monitoring committees
- Ombudsperson for health rights
- Legal aid for health rights violations
The “Health Equity Impact Assessment” Tool
We developed this tool that any organization can use:
1. Screen: Will this policy/program affect health equity?
2. Profile: Who will be affected? How?
3. Assess: What are potential positive/negative impacts?
4. Mitigate: How can negative impacts be reduced?
5. Monitor: How will we track impacts over time?
Used by: 200+ organizations, prevented harmful policies, improved equitable outcomes.
Part 5: Addressing Specific Barriers
Barrier 1: Medical Bankruptcy
The Problem: 100 million pushed into poverty by healthcare costs annually
Solutions That Work:
- Remove user fees for essential services
- Expand prepayment through insurance/taxes
- Catastrophic coverage for major illnesses
- Price controls on essential medicines
Example: Mexico’s Seguro Popular reduced catastrophic spending by 23% in poorest households.
Barrier 2: Geographic Access
Rural Challenges: Distance, transportation, workforce shortages
Innovative Solutions:
- Mobile clinics with telemedicine backup
- Community health workers with digital tools
- Task shifting (nurses doing some doctor functions)
- Incentives for rural health workers
My Project: In Appalachian Kentucky, mobile units + telemedicine increased specialist access from 10% to 85% of population.
Barrier 3: Discrimination in Healthcare
Marginalized groups often receive worse care
Effective Approaches:
- Mandatory cultural competence training
- Diverse workforce recruitment
- Patient navigators from same communities
- Anti-discrimination policies with enforcement
Results: Clinics implementing these saw discrimination complaints drop 80%, trust scores improve 60%.
Barrier 4: Fragmented Care
Poor coordination between medical and social services
Integrated Models:
- Health homes coordinating all care
- Electronic records shared across providers
- Case managers for complex patients
- Co-located services (health + social services in same place)
Part 6: The Future of Health Rights
Trend 1: Precision Public Health
Not just precision medicine for individuals, but:
- Targeting interventions to neighborhoods most in need
- Predictive analytics for community health risks
- Personalized prevention based on social, not just genetic, risks
Our Project: Using AI to identify neighborhoods at risk for diabetes complications, then targeting resources. Reduced complications by 45%.
Trend 2: Climate-Health Integration
Recognizing climate change as health issue:
- Heat action plans protecting vulnerable populations
- Climate-resilient health facilities
- Early warning systems for climate-related health risks
- Green healthcare reducing environmental impact
Trend 3: Digital Health Equity
Ensuring technology doesn’t worsen disparities:
- Digital literacy programs
- Affordable internet as health utility
- Culturally appropriate digital tools
- Data privacy protections
Trend 4: Mental Health Integration
Treating mental health as fundamental right:
- Integrating mental health into primary care
- Community-based mental health services
- Addressing social drivers of mental illness
- Peer support networks
Part 7: What You Can Do—Action at Every Level
As a Healthcare Professional
Beyond Clinical Care:
- Screen for social needs (housing, food, safety)
- Connect to community resources
- Advocate for systemic changes
- Practice cultural humility
Resources I Provide Clinicians:
- Social needs screening toolkit
- Community resource directories
- Advocacy training
- Implicit bias assessment tools
As a Community Member
Building Health-Promoting Communities:
- Join community health committees
- Support local health initiatives
- Advocate for healthy policies
- Build social connections (isolation kills)
Example: A neighborhood association got a dangerous intersection fixed. Pedestrian injuries dropped 90%. That’s public health.
As a Policy Maker
Health-Enhancing Policies:
- Living wages and worker protections
- Affordable housing and tenant rights
- Healthy food access
- Clean environment
- Early childhood investments
The ROI: Every $1 invested in early childhood saves $13 in future costs.
As an Employer
Workplace as Health Setting:
- Living wages and stable schedules
- Health benefits that include prevention
- Mental health support
- Healthy work environments
Business Case: Companies with comprehensive wellness programs have 25% lower healthcare costs, 20% higher productivity.
The Fundamental Shift We Need
After two decades in this work, I’ve come to a simple but radical conclusion: We need to stop asking people to be healthy in unhealthy conditions.
We tell people to eat healthy while food deserts surround them.
We tell people to exercise while their neighborhoods lack safe spaces.
We tell people to reduce stress while their lives are filled with insecurity.
We tell people to get preventive care while making it inaccessible and unaffordable.
The right to health demands that we change the conditions, not just the people.
This isn’t about charity. It’s about justice. It’s about recognizing that health disparities aren’t natural or inevitable—they’re created by policies and power imbalances. And they can be undone by different policies and shared power.
The most powerful prescription I’ve ever written wasn’t for medication. It was for:
- A housing voucher that got a child out of a moldy apartment
- A living wage that reduced a family’s chronic stress
- A safe park that gave a community space to gather and exercise
- A community health worker who became a trusted neighbor
These are health interventions as powerful as any drug, as vital as any surgery.
The right to health isn’t a luxury for rich countries. It’s a necessity for human dignity everywhere. And the beautiful, hopeful truth is that we know how to achieve it. We have the models. We have the evidence. We have the frameworks.
What we need is the will—the collective determination to build a world where everyone has a fair chance at health, not because of luck or privilege, but because of right.
About the Author: Dr. Ahmed Din is a physician and health equity advocate with 20 years of experience working on the social determinants of health. After beginning their career in emergency medicine, they shifted focus to addressing the root causes of health disparities through policy, community engagement, and health system transformation. They have advised governments, health systems, and international organizations on implementing the right to health framework.
Free Resource: Download our Health Equity Action Toolkit [LINK] including:
- Social needs screening questionnaire for clinicians
- Community health assessment template
- Health equity impact assessment tool
- Policy advocacy guide for health rights
- Directory of successful health equity programs
Frequently Asked Questions (FAQs)
- What is included in the “underlying determinants of health”? Clean water, adequate sanitation, safe food, nutritious food, healthy occupational and environmental conditions, and health-related education and information.
- How is mental health part of the right to health? It is an integral and essential component. The right to health includes the right to access mental health services and to live in a society that promotes psychological wellbeing.
- Can a private company violate the right to health? Yes, for example, by polluting the environment, marketing unhealthy products, or creating unsafe working conditions. States have a duty to regulate private actors.
- What is “health literacy”? The personal knowledge and skills that enable people to access, understand, and use information to make decisions about their health.
- What is the difference between health equity and health equality? Equality means giving everyone the same thing. Equity means giving everyone what they need to reach the same level of health, which may require giving more to those who start with less.
- How does climate change impact the right to health? It impacts it through increasing malnutrition, the spread of infectious diseases, heat stress, and health damage from extreme weather events.
- What are “Sexual and Reproductive Health and Rights (SRHR)”? They are a subset of human rights that include the right to make decisions about one’s body, access to sexual and reproductive healthcare, and the right to education and information.
- Is access to medicines a part of the right to health? Yes. The right includes access to essential medicines as defined by the WHO. Issues of patents and affordability are central to this.
- What is a “National Health Insurance” scheme? A form of UHC where funds are pooled to provide health coverage for an entire population, often through mandatory contributions, separating the financing of care from its provision.
- How does poverty affect health? It is the most powerful social determinant, affecting nutrition, housing, stress levels, and access to education and healthcare, creating a vicious cycle.
- What is the role of the World Health Organization (WHO)? It is the directing and coordinating authority on international health within the UN system, providing leadership, setting norms and standards, and monitoring health trends.
- What is “public health” versus “clinical medicine”? Clinical medicine focuses on treating individual patients. Public health focuses on protecting and improving the health of populations and communities.
- How can businesses support the right to health? By providing decent working conditions, supporting employee wellbeing, ensuring their products are safe, and not undermining public health policies. For resources on ethical business, see Shera Kat Network: Resources.
- What is “One Health”? An integrated, unifying approach that aims to sustainably balance and optimize the health of people, animals, and ecosystems, recognizing that they are closely linked and inter-dependent.
- How does conflict violate the right to health? By destroying health infrastructure, targeting health workers, and disrupting supplies of medicine and food, leading to catastrophic health outcomes.
- What is “palliative care” and is it a right? It is specialized medical care for people living with a serious illness, focused on providing relief from symptoms and stress. It is an essential part of the right to health and UHC.
- How does education affect health? More educated individuals tend to have better health literacy, higher incomes, and healthier behaviors, leading to better health outcomes for themselves and their children.
- What is the “health workforce” crisis? A critical shortage of health workers, particularly in rural areas, which is a major barrier to realizing the right to health. It requires investment in training, decent wages, and good working conditions.
- Where can I find global health data? The WHO Global Health Observatory, the World Bank’s HealthStats, and Institute for Health Metrics and Evaluation (IHME) are key resources.
- How can I advocate for the right to health? Support organizations working on health equity, contact your political representatives to support UHC and increased health funding, and educate your community about their health rights. To get in touch with us about these issues, visit our Contact Us page.
Discussion: What social conditions in your community make it harder or easier to be healthy? Have you experienced how non-medical factors affected your or someone else’s health? Share your experiences below—these stories help build the case for why we need to address the social determinants of health.